Rapid Recanalization of Right MCA Occlusion with Hemo’s 8F EmerAX / TracLine LDP (088-100) Large Bore Intermediate Catheter
Surgeon Introduction
Ruan Zhong Fan The First Affiliated Hospital of South China University
Deputy Chief Physician of the Department of Neurology, First Affiliated Hospital of South China University, National Resident Training Backbone Teacher, mainly engaging in clinical and research work regarding cerebrovascular diseases.
Completed the neuro-interventional specialty training in Chang Hai Hospital of Naval Military Medical University and attended the special training in direct aspiration thrombectomy in Xin Qiao Hospital of Army Military Medical University. He specializes in cerebrovascular treatment and long term cerebral disease management, and has rich experience in interventional treatment of large vessel occlusive stroke and interventional treatment of cerebrovascular disease via trans-radial means.
Oversaw one project from Hunan Provincial Health Committee, Hengyang Science and Technology Bureau each, and South China University’s educational reform. He has published more than 10 papers, including 5 SCI papers. He has GCP qualification for drugs and medical devices and is responsible for one medical device clinical trial (sub-centre PI) and one drug clinical trial (sub-center PI).
Case information
Patient chief complaint: Impaired left limb mobility for 2 hours Current medical condition: 2 hours ago, the patient suddenly developed left-sided limb weakness, complete paralysis, slurred speech, and had drooping mouth with no obvious cause. He was admitted to the emergency room, and a CTA of the head and neck indicated occlusion of the right MCA. Medical history: Hypertensive disease grade 3 (very high-risk group), dilated cardiomyopathy, atrial fibrillation. Physical examination: NIHSS 16, GCS 3+5+6=14, drowsiness, poor dysarthria, bilateral gaze to the right, shallow left nasolabial fold, left limb muscle strength grade 0, left limb hyperalgesia, positive left baroreflex sign. Diagnosis: 1. Acute cerebral infarction with right middle cerebral artery occlusion (cardiogenic embolic type) 2. Dilated cardiomyopathy, atrial fibrillation 3. Hypertensive disease grade 3 (very high risk group)
Treatment Process (AIS CASE)
Preoperative Images
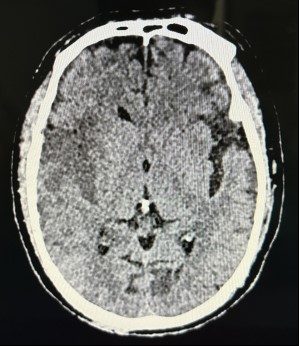
Figure 1: Intracranial plain CT scan: left parieto-occipital subdural hematoma
Figure 2: CTA of head and neck: right MCA occlusion
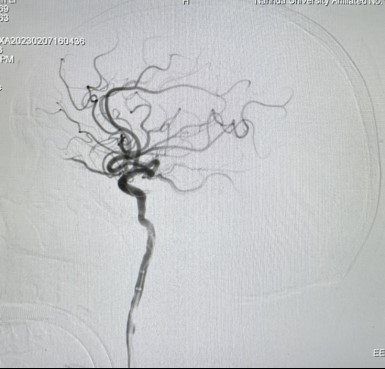
Figure 3: DSA: right MCA M1 segment occlusion
Preoperative Breakdown
Objective of the operation: To achieve effective recanalization of the occluded vessel as soon as possible Key points of operation: The 8F intermediate catheter EmerAX / TracLine LDP (088-100) reaches high up the vessels; the stent anchors onto the vessel; intermediate catheter contacts the thrombus to achieve effective thrombectomy via suction and pulling at the same time. Operation difficulties/risks: Whether the intermediate catheter can come into contact with the thrombus to achieve effective thrombectomy via pulling and suction at the same time, is the key to rapid revascularization, and whether the LDP can reach high into the vessels is an important factor for the intermediate catheter to contact the thrombus. If the thrombus escapes, it can cause occlusion of the distal vessels, and repeated pulling to remove the thrombus increases the risk of bleeding and dissection. Other: The patient had a subdural hematoma, which was contraindicated for thrombolysis, so no thrombolysis was performed. The patient has dilated cardiomyopathy, atrial fibrillation and poor cardiac function. Rapid recanalization can reduce intraoperative risk and anesthesia coverage. Postoperative management is important.
Operation Procedures
Hemo’s 8F EmerAX / TracLine LDP (088-100) is located in C2 segment, in the selected artery. The stent is released. Next, utilising the support that EmerAX / TracLine LDP provides, along with the anchoring effect of stent retriever, the Intermediate Catheter will be able to cross the siphon bend into the M1 region.
EmerAX / TracLine will be furthered delivered into the C4 segment where the SWIM technique is employed to retrieve the blood clot. Remove the stent retriever, do not rush to inject contrast dye. With the intermediate catheter in hand, aspirate once. Contrast dye will be later injected to confirm recanalization of vessel.
Figure 5: 24-hour postoperative cranial CT: no Hemorrhage in the right midbrain lesion area
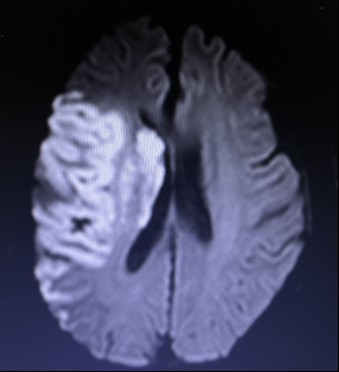
Figure 6: Postoperative day 3 cranial MRI: right frontal and temporoparietal brain infarction
Figure 7: Postoperative day 3 cranial MRA: right MCA lumen is patent
Follow-Ups
The patient was discharged with a NIHSS score of 3 at 24 hours postoperatively and a NIHSS score of 2 on postoperative day 7.
Case Summary
Case characteristics: The patient was a typical case of middle cerebral artery embolism, and the extensive reach of the EmerAX / TracLine 088 guaranteed effective extraction combined with embolization for rapid recanalization and hence, allowed for significant patient benefit.
Key points during preoperative evaluation: 1. determination of the nature of the lesion: the patient had atrial fibrillation and the lesion was in the M1 segment of the middle cerebral artery, consistent with signs of thrombus occlusion; 2. CTA of the head and neck showed a tortuous siphon of the internal carotid artery, and whether the intermediate tube could pass through the siphon bend and then reach the thrombus was the key to the success or failure of the operation.
Key points on operation technique: 1. Extensive reach of EmerAX / TracLine LDP (088-100), a Hemo 8F catheter; 2. The intermediate catheter passes through the siphon and then contacts the thrombus.
Equipment use technique: When using the Hemo 8F EmerAX / TracLine LDP (088-100), do not attempt to deliver the catheter to target site in one step. If the path is tortuous, use tri-axial technique where intermediate catheter and microcatheter are used in combination. This will aid in achieving a high placement for EmerAX / TracLine LDP.
Reference: [1] Zi W, Qiu Z, Li F, et al. Effect of Endovascular Treatment Alone vs Intravenous Alteplase Plus Endovascular Treatment on Functional Independence in Patients With Acute Ischemic Stroke: The DEVT Randomized Clinical Trial[J]. JAMA. 2021,325(3):234-243.
About Hemo Bioengineering
Hemo Bioengineering Co., Ltd. (hereinafter referred to as “Hemo”) officially commenced operations in 2017. Hemo’s global headquarters are located in Singapore, with R&D centers in US, Singapore and China. The company maintains long-term collaborations with US-based R&D laboratories to ensure the design of new products aligns with cutting-edge global technologies.
Hemo is dedicated to leveraging global high-quality R&D, production, clinical, and academic resources to provide innovative vascular and neurological interventional products. These products aim to serve doctors and patients worldwide by offering comprehensive interventional treatment solutions for cerebrovascular diseases such as ischemic stroke, hemorrhagic stroke, and intracranial vascular stenosis.
Cookies
Please note that your use of this website is governed by your acceptance of our Terms of Use. We also use cookies on our website to understand the usage patterns of visitors, so that we may be able to enhance their browsing experience and improve the website and/or our services. We may also allow certain third parties to place cookies on our website to collect information about your online activities on our website and across different websites you visit over time. Please click here for more information about our Cookie Policy.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.