Percutaneous MCA thrombectomy using Hemo’s Aspiration Catheter
Surgeon's profile

Xin Gou Qiang
Shandong Sunshine Ronghe Hospital
Shandong Sunshine Ronghe Hospital’s Associate Chief Physician, Masters postgraduate
Dr Xin served as a member of the Shandong Provincial Cerebrovascular Disease Prevention and Control Committee, the Medical Device Management Committee of the Chinese Medical Education Association, a member of the Weifang Medical Doctor Association Brain Stroke TCM Branch, a member of the Weifang Preventive Medicine Association’s First Neurological Disease Prevention and Control Professional Committee, and a member of the Weifang Medical Association’s Third Cerebrovascular Disease Professional Committee.
He mainly engages in the works of neuro intervention, carrying basic treatment for common diseases, and frequently occurring diseases in neurosurgery. He was also responsible for assisting the hospital to develop the stroke emergency green channel, carrying out carotid angioplasty and stent implantation, intracranial hematoma removal, decompressive craniectomy, ventricular drainage, aneurysm clipping, aneurysm endovascular treatment, arteriovenous malformation surgery and endovascular treatment. Over the past five years, more than 1000 patients have been treated, more than 500 surgeries have been performed, and more than 200 tertiary and tertiary interventional surgeries have been completed independently under the guidance of the director, ensuring the satisfaction of the patients, promoting the development of departments, and adding colour to the hospital.
He has also published 5 papers in professional core journals.
Case information
Chief Complaint: Left limb weakness was found for more than 1 hour.
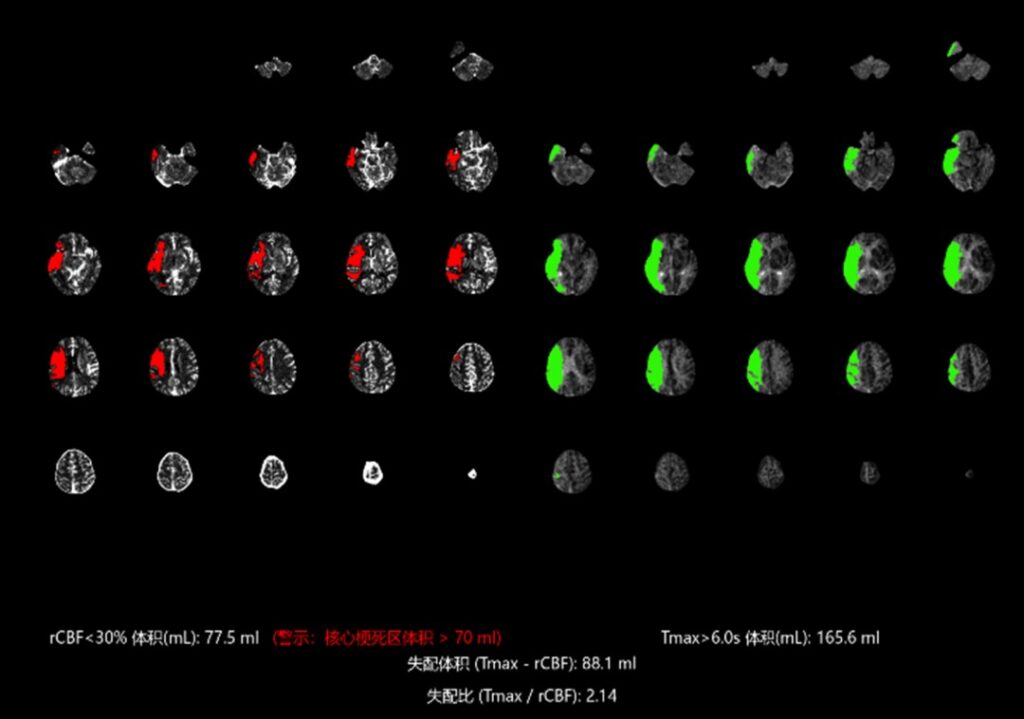
Current Medical Condition: The patient woke up at 2:40 p.m. on June 7, 2022 and found that his left limb was weak, unable to hold and lift, speech was unclear, mouth angle was skewed. Family members and patient explained that there was no obvious discomfort before going to bed 6 hours ago, so he went to our hospital for emergency treatment at 3:40 p.m. and did not carry out thrombolysis because the time of onset was unknown. At 4:05, brain CT enhanced perfusion showed that the blood flow in the right middle cerebral artery was decreased, Tmax>6s 165.6ml, and core infarction 77.5ml.
Past Medical History: Has a history of “Cerebral infarction” half a year ago without obvious sequelae.
Physical Examination on Admission: NIHSS 11 points, mRS: 5 points, lethargy, unclear speech, normal understanding, both eyes staring at the same direction to the right, no nystagmus, shallow nasolabial groove on the left, tongue extension to the left, left limb muscle strength grade 0, left lower limb pathological sign positive.
Diagnosis: Acute cerebral infarction.
Treatment Process (AIS CASE)

Preoperative Images
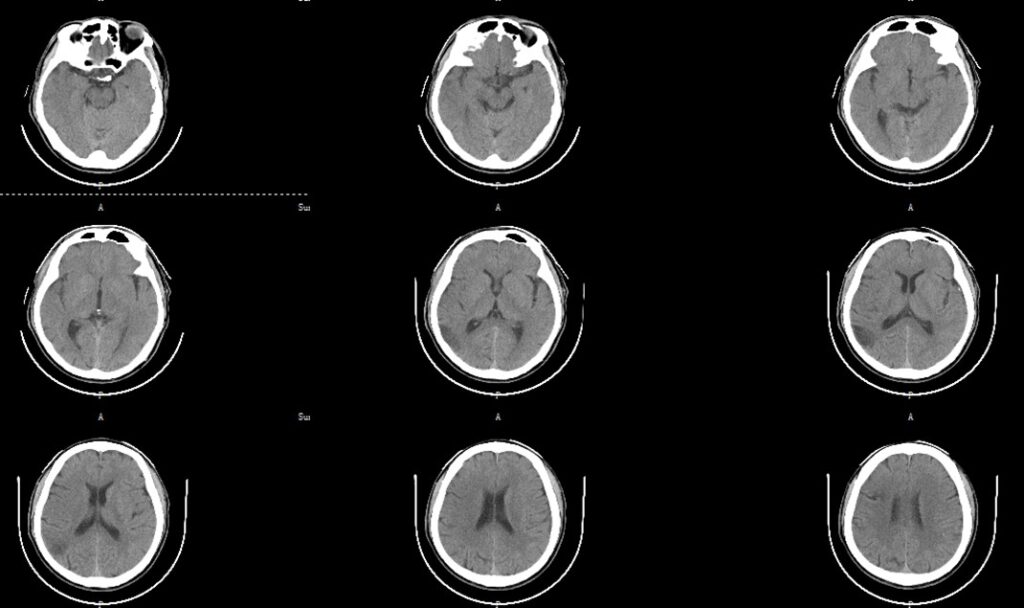
Head CT plain scan: multiple cerebral infarction lesions in right frontal lobe and temporo-occipital lobe.
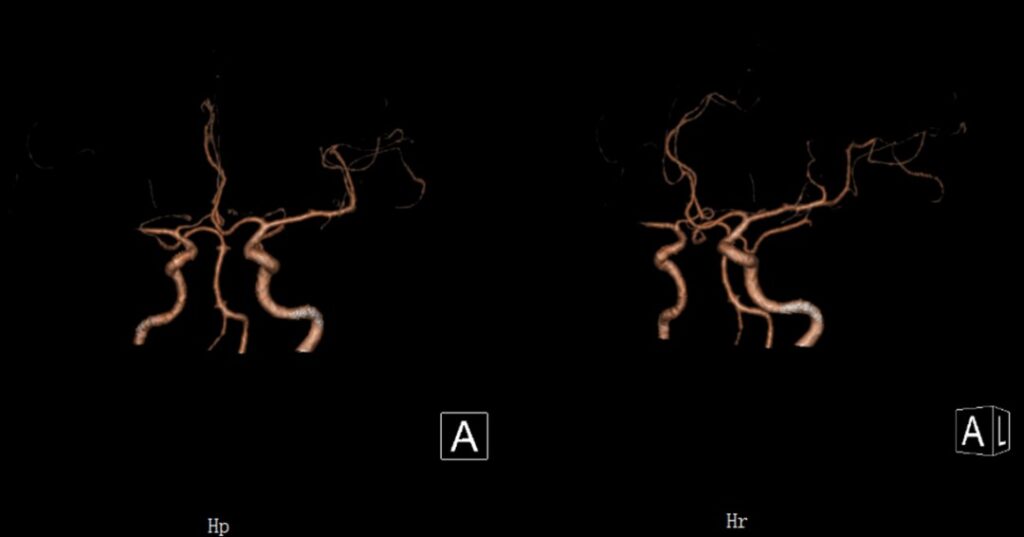
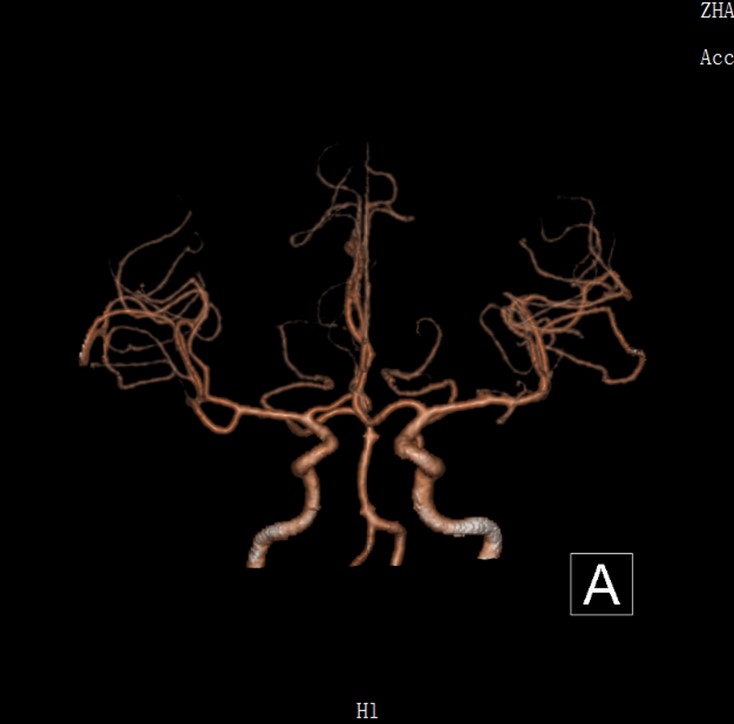
Craniocerebral artery CTA: The examination showed that the right MCA was occluded.
CT perfusion imaging: the right fronto temporo-occipital region of interest suggests right hypoperfusion, poor perfusion.
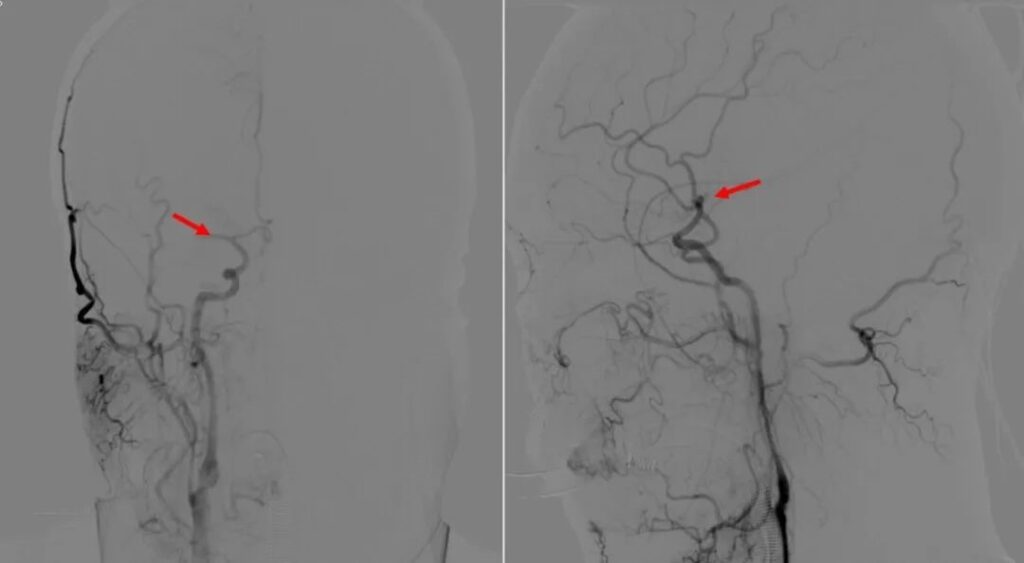
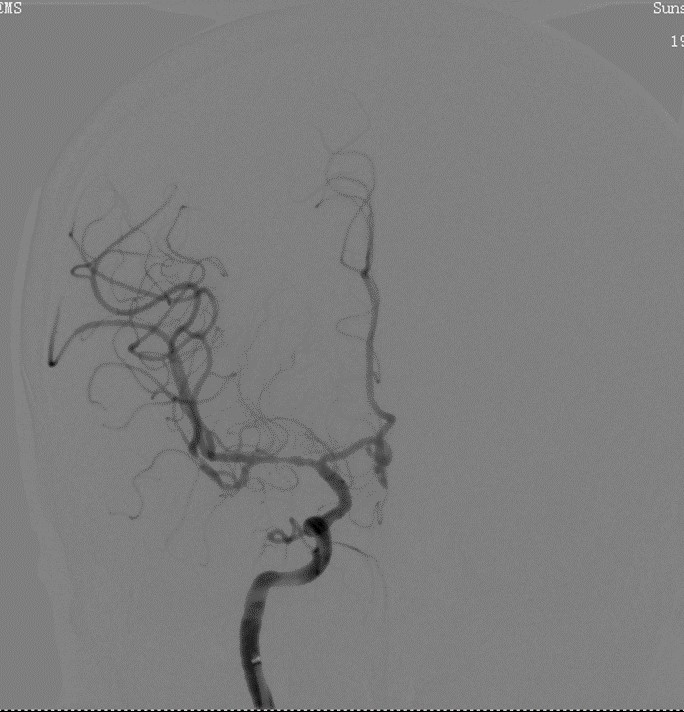
DSA: The anteroposterior and lateral angiography of the right ICA showed the right MCA occlusion.
Preoperative Breakdown
Objective of the operation:
To achieve the recanalization of the right MCA, ensure the blood supply of the MCA blood supply area, and improve the state of ischemia and hypoxia.
Key points of operation:
First, pass the microcatheter and micro-guide wire through the occlusion of the right MCA, and introduction of the contrast medium shows that the microcatheter is in the true lumen of the blood vessel; Hemo’s 065-127 aspiration catheter can be delivered pass the carotid siphon, due to the catheter’s good support and flexibility. Release the stent retriever and remove the thrombus by utilising the combination method of providing aspiration on the thrombus using the aspiration catheter while pulling stent retriever concurrently.
Operation difficulties/risks:
Trying to pass the microcatheter and micro-guide wire through the occlusion of the right MCA to ensure that the microcatheter is in the true lumen of the blood vessel.
Others:
Achieve blood vessel recanalization as soon as possible, stabilize blood pressure during and after operation, and reduce the risk of high perfusion and bleeding.
Operation Procedure
Introduction of the contrast medium shows that the microcatheter is in the true lumen of the MCA.

Hemo’s 065-127 aspiration catheter was delivered pass the carotid siphon and provided aspiration of the thrombus. Angiography with constant medium showed the distal part of the MCA and that the stent retriever was expanded well.

Post Operative Images
Anterior and lateral internal carotid angiography after thrombectomy showed that the reperfusion of the MCA was achieved.

After thrombectomy, the brain CT was re-examined, and no hyper perfusion or haemorrhage was found.

Follow Up
Brain MRI was re-examined 2 months after operation. Multiple chronic cerebral infarction foci were found in the right fronto temporo-occipital lobe.

Brain CTA was re-examined 2 months after operation, and good blood flow in right MCA was still observed.
Clear consciousness, clear speech, normal understanding, normal memory and orientation, normal rough measurement field of vision, free movement of both eyes, no nystagmus, shallow nasolabial groove on the left, tongue extension to the left, negative test of bilateral limb paresis, normal muscle strength of both limbs, and no pathological signs of both lower limbs. Patients can engage normally in daily work.
Case Summary
Case characteristics:
The patient has an acute onset, combined with symptoms and examination, considering the large vascular lesions, improving the perfusion examination and evaluation in the emergency, making a clear diagnosis, and giving mechanical thrombectomy treatment in the emergency.
Key points during preoperative evaluation:
Plain CT scan of the patient’s brain indicates cerebral infarction; Brain CTA and perfusion imaging showed that the right MCA was occluded, the blood supply of the MCA was greatly insufficient, and there was a mismatch in the infarcted area.
Key points on operation technique:
Pass the microcatheter and micro-guide wire through the right MCA occlusion to ensure that the microcatheter is in the true lumen of the blood vessel.
Equipment use technique:
Hemo’s aspiration catheter can be easily delivered pass the carotid siphon due to the catheter’s exceptionally good support and flexibility. The design of the bevel tip at the end of the catheter also allows a larger thrombus contact area, which can better grasp the thrombus, increasing the suction efficiency.
Reference:
Chinese expert consensus on endovascular treatment of acute large vessel occlusive ischemic stroke (revised in 2019)
The Product
Hemo’s Aspiration Catheter has the following advantages:
1. The largest contact area of the head end added by the large inner cavity and the inclined plane has the highest suction efficiency.
2. Patented structure design, stronger anti-negative pressure capacity of the catheter, which will not be easily deflated.
3. Unique hydrophilic coating design ensures smoother transportation.
4. 3F~6F models provide more options for surgery.
About Hemo
Hemo Biotechnology Co., Ltd. (referred to as “Hemo”) officially commenced operations in 2017. Hemo’s global headquarters is in Singapore, with research and development centers in both Singapore and China. It collaborates with long-term partners in the United States to focus on new product design and keep abreast of cutting-edge global technologies.
Hemo is dedicated to integrating high-quality global research and development, production, clinical, and academic resources to provide innovative vascular and neurointerventional products for patients and medical professionals. It aims to offer comprehensive intervention solutions for cerebrovascular diseases, including ischemic stroke, hemorrhagic stroke, and intracranial vascular stenosis.