Deputy Director of Neurology and Comprehensive Interventions
Member of Brain Disease Branch of the Chinese Academy of Gerontology and Gerontology
Standing Committee of the Brain Vascular Intervention and Emergency Interventions Branch of the Chongqing Stroke Society
Standing Member of the Division of Neurology of the Chongqing Physicians Association
Member of the Youth Committee of the Stroke Society of Chongqing
Member of Chapter of Neuroimmunology of the Southwest Stroke Society
Member of The Chapter of Interventional Medicine of the Association of Social Medical Institutions of Chongqing
Awarded the title “Expert in the prevention and treatment of cerebrovascular disease” in Chongqing. Specializes in emergency and elective interventional surgery for ischemic cerebrovascular disease and in interventional surgical treatment for peripheral vascular disease. Studied neuro-interventional surgery at Newbridge Hospital, affiliated with the Army Medical College. Published several papers.
Case information
Chief Complaint: 63 year old woman, non-speech and weakness in right limb for 4 hours.. Current Medical Condition: 4 hours before admission, her family noticed that she was unable to speak, had impaired hearing and understanding, had no movement of the right side of her body, and had an askew mouth. Unconscious disorder, limb twitching, intermittent wheezing, no vomiting, fearless cold, wheezed and wheezy, a few coughs and sputum, persistent symptoms. Emergency admittance into our hospital. Past Medical History: Hypertension, diabetes mellitus for more than 7 years, no regular medication. History of lower limb deep vein thrombosis 6 yrs ago, which improved after treatment. Physical Examination on Admission: Temperature 36.9 ° C P: 104 / d R: 19 / d BP: 182 / 100 mmHg. Both lungs exhibited crackling sounds with fluid accumulation, heart rhythm was regular, and valve auscultation revealed no irregularities. The abdomen was soft with no tenderness, and there was no pain upon palpation of the abdominal area. Lower extremities were without signs of edema. Neurological examination: Revealed somnolence and mixed aphasia. Partial body coordination, with symmetric bilateral frontal striations present. Eyes were deviated to the left, with pupils equal in size (0.3 cm in diameter), round, and reactive to light. No nystagmus observed. Right nasolabial fold was shallow, and no cervical obstruction. Muscle strength graded 0 on right side and 5 on left side. Physical examination findings were inconclusive, and a positive Babinski sign was noted on the right. NIHSS score: 21 points (consciousness 1, questioning 2, command 2, gaze 1, facial paralysis 2, left upper limb movement 4, left lower limb movement 4, language 3, articulation 2). mRS Rating: 0 points. ECG: sinus tachycardia, ST segment low pressure. Random finger blood sugar: 10.5 mmol / L.
Preoperative imaging and diagnosis
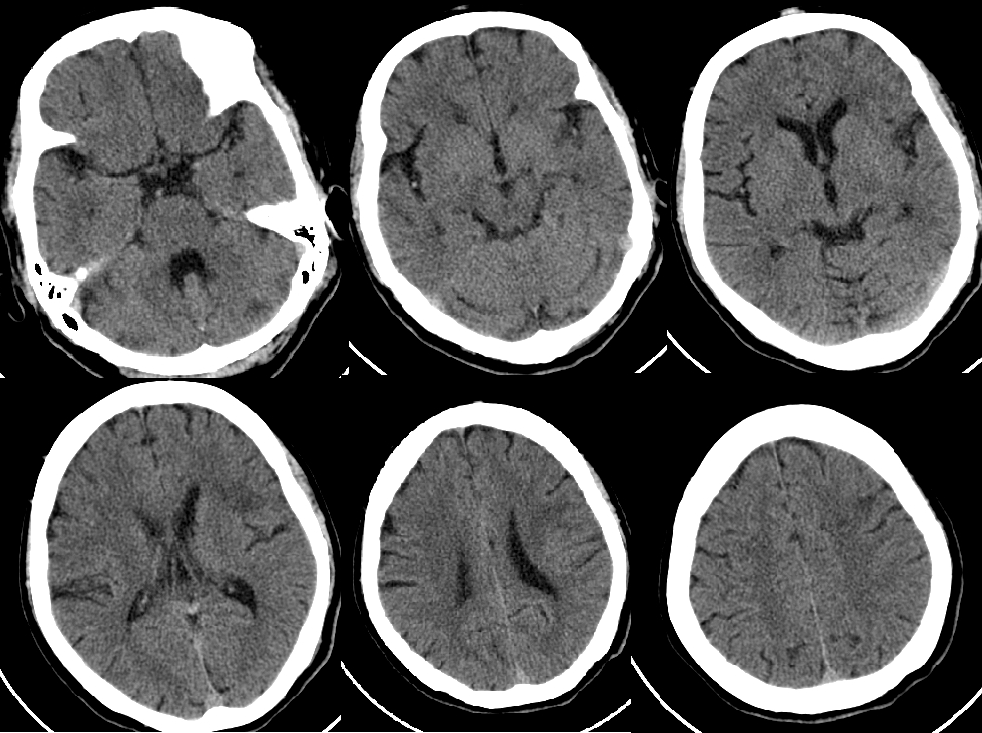
NCCT: ASPECTS Score 8
Head MRI: DWI (+), FLAIR (+)
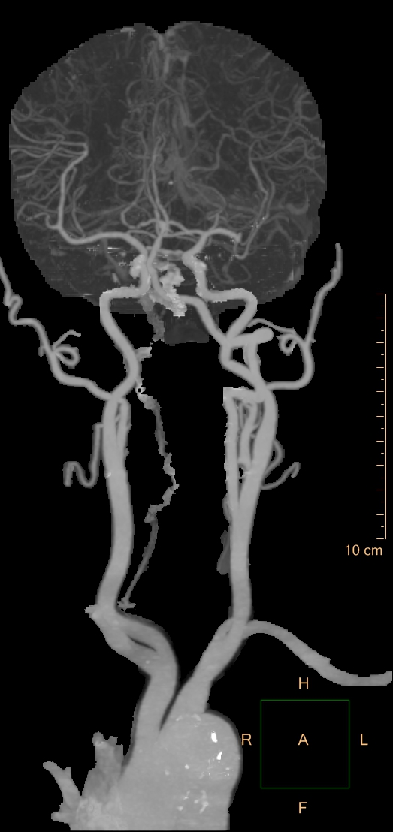
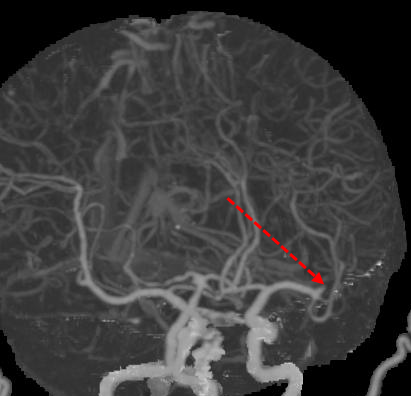
Head and Neck CTA: Occlusion of the Origin of the LM2 Upper Trunk
Diagnosis
1. Acute cerebral infarction
2. LM2 upper stem initiation occlusion
3. High Blood Pressure Grade 3 (Very High Risk)
4. Type-2 diabetes mellitus
Diagnosis and treatment strategies
1. The patient experienced a stroke while conscious, with MRI findings showing positive diffusion-weighted imaging (DWI) and fluid-attenuated inversion recovery (FLAIR). Administration of rTPA was less beneficial. Clinical symptoms were severe, with an NIHSS score of 21. The infarct core was small (NCCT: ASPECTS score of 8), and there was moderate vascular occlusion at the origin of the upper trunk of LM2.
2. The benefit of emergency endovascular treatment in patients with acute moderate vascular occlusion remains uncertain. After careful screening and assessing the risk-benefit ratio, emergency endovascular treatment may offer a better treatment option. However, further evidence from randomized trials is required (Class IIb recommendation, Level B)*.
3. The family members opted for intravascular treatment after providing informed consent.
*Chinese guidelines for endovascular treatment of acute ischemic stroke 2023 [J].Chinese Journal of Stroke, 2023, 18 (06): 684-711.
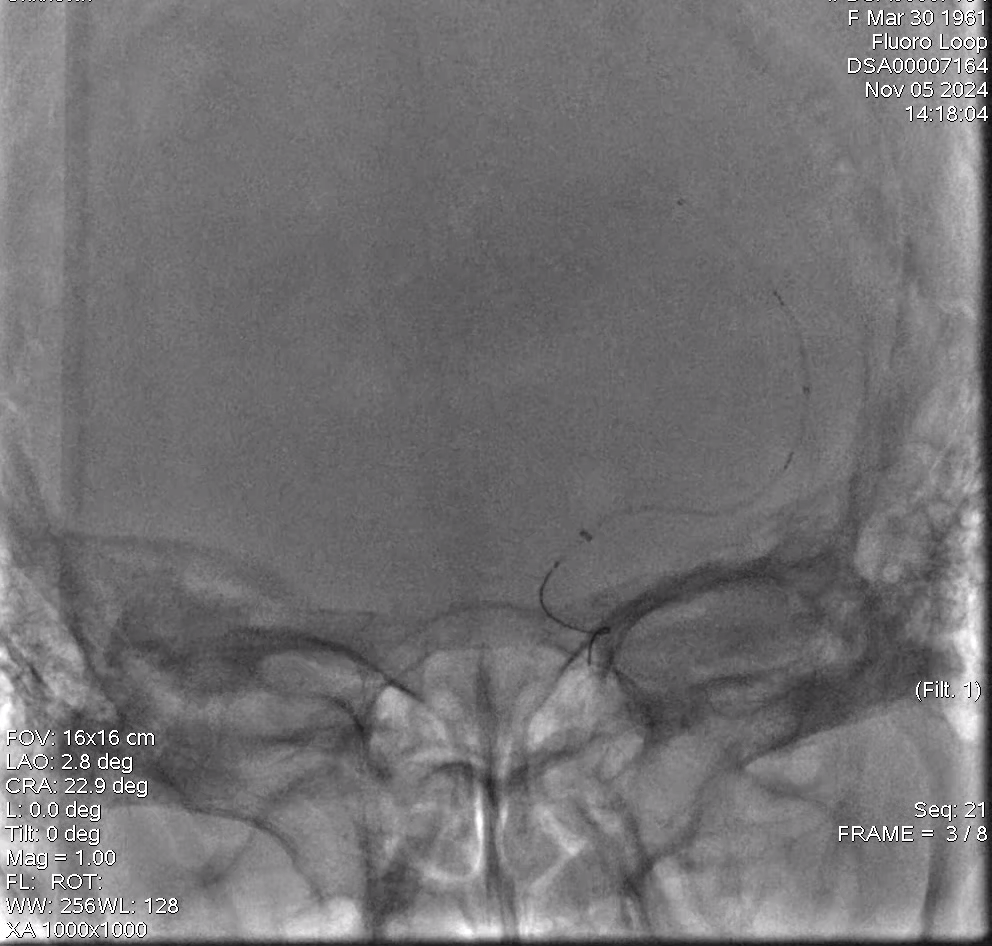
Preoperative Images
Preoperative Imaging
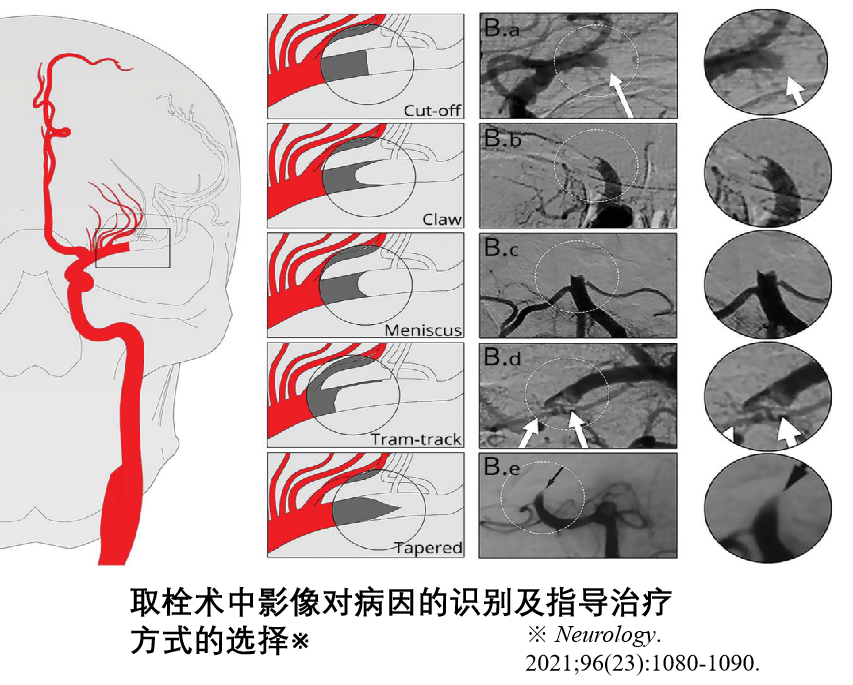
Considering ICAS lesions, balloon dilation is performed first. The decision to proceed with mechanical thrombectomy will depend on the patient's condition.
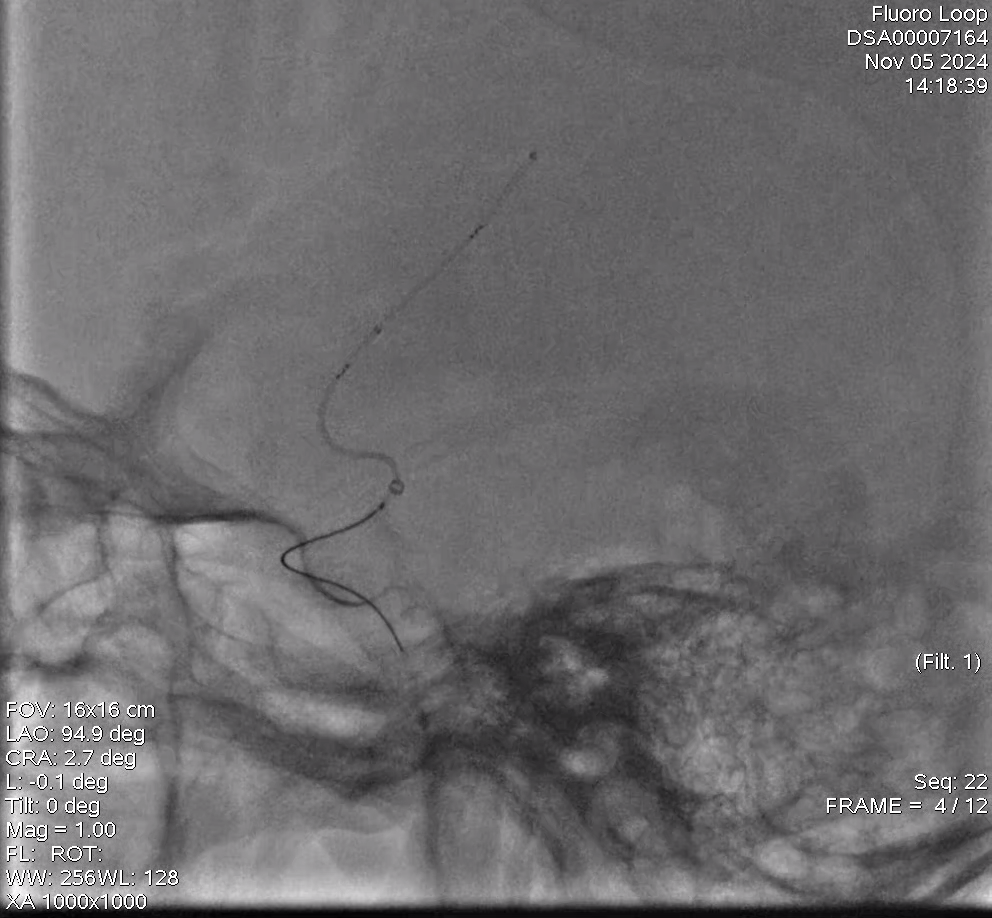
Operation Procedure
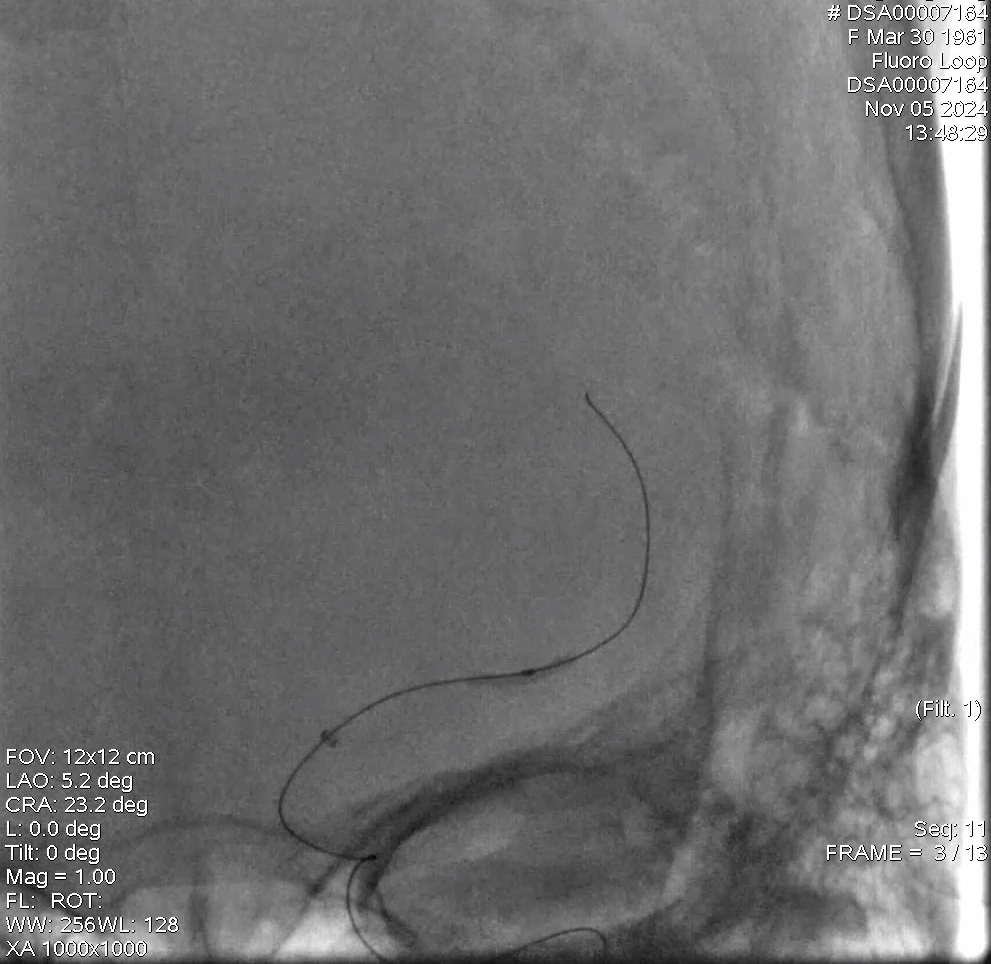
1.5 × 15mm balloon expansion
After balloon dilation, a blood clot was identified locally, prompting the decision to use a stent for clot removal.
Using a Mountix 021" microcatheter, the CerebrAX/FlexTake 4mm*40mm stent retriever was delivered to the M2 segment of the left MCA. The microcatheter was slowly retracted to release the stent retriever at the M1-M2 junction. Imaging showed recanalization of the proximal segment, with the distal blood vessels becoming visible.
The SWIM technique achieved first-pass recanalization. Angiography revealed complete recanalization of the upper trunk of the left MCA, with forward blood flow reaching mTICI grade 3.
Post Operative Images
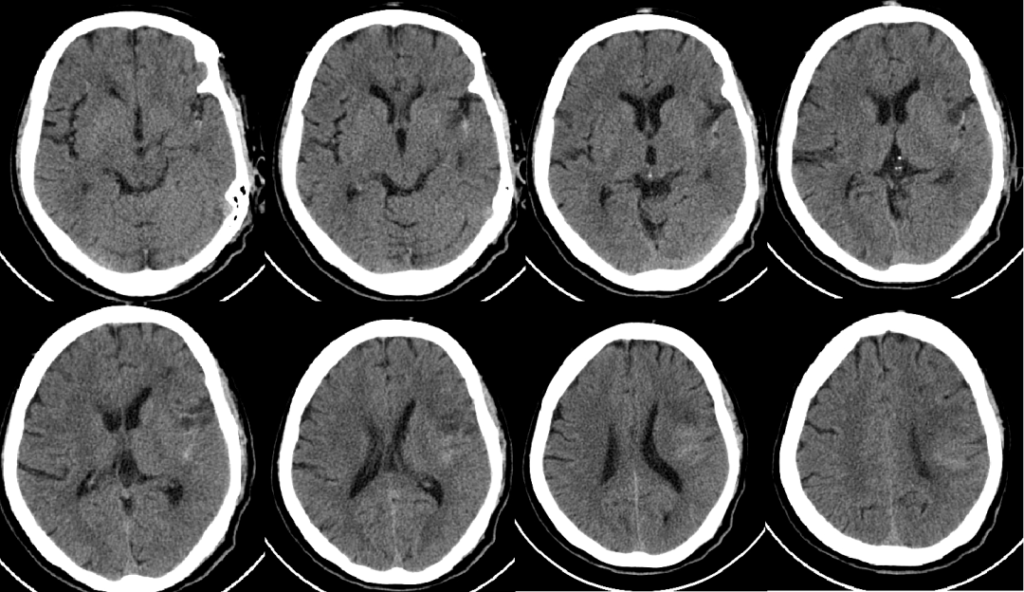
A CT scan of the head taken on the second day post-surgery showed cerebral infarction in the left insular lobe and the centrum semiovale, with mild hyperdensity, possibly indicating opacifier extravasation.
Discharged after 2 weeks hospitalization
Neurological assessment: The patient is alert with clear speech and able to answer basic questions. Memory and numeracy are slightly impaired. Bilateral pupils are round, approximately 3 mm in diameter, and reactive to light. Eye movements are intact in all directions, with no nystagmus. Right-sided central paralysis observed. Tongue protrudes symmetrically. Limb strength is graded 4+ on the right and 5 on the left. Babinski sign is absent.
NIHSS score: 1 (facial paralysis 1)
Guidelines for medications upon discharge
Aspirin enteric-coated tablets 100mg once daily, Atorvastatin calcium tablets 20mg at night, Amlodipine Besylate tablets 2.5mg once daily, Metformin tablets 515mg twice daily, Dapagliflozin tablets 10mg once daily, Butylphthalide soft capsules 0.2g as prescribed.
Case Summary
1. Case characteristics:
An elderly woman who experienced a stroke upon waking.
The clinical symptoms are severe, the infarct core is small, vascular occlusion is moderate, and the surgical risk is high.
The risk of damage and bleeding is high following vessel reperfusion.
2. Preoperative evaluation:
Preoperative evaluation: Emergency CTA and MRI of the head and neck to rule out cerebral hemorrhage, assess the aortic arch and cervical vascular conditions, identify the occlusion site, and determine the infarcted area, in order to evaluate the surgical risk.
Preoperative evaluation: Optimize blood routine, coagulation profile, and blood transfusion if necessary. Perform ECG, chest CT, and address any surgical contraindications.
3. Surgical technique highlights:
Based on preoperative CTA and intraoperative DSA, evaluate the surgical approach and strategically plan the procedure;
SWIM technology helps minimize the risk of thrombus dislodgement and enhances the recanalization rate.
In the application of the SWIM technique, the suction tube is positioned to make maximum contact with the thrombus, enhancing the suction effect. The stent retrieval is slow and continuous, which helps reduce the risk of thrombus dislodgement and improves the recanalization rate.
4. Device usage advice: For patients with tortuous vessels, the CerebrAX/FlexTake stent retriever offers balanced radial support and flexibility, ensuring excellent delivery performance and strong clot retrieval capability. It provides a higher hand reflux rate, reducing the risk of clot dislodgement.
The Product
About Hemo
Hemo Biotechnology Co., Ltd. (referred to as “Hemo”) officially commenced operations in 2017. Hemo’s global headquarters is in Singapore, with research and development centers in both Singapore and China. It collaborates with long-term partners in the United States to focus on new product design and keep abreast of cutting-edge global technologies. Hemo is dedicated to integrating high-quality global research and development, production, clinical, and academic resources to provide innovative vascular and neurointerventional products for patients and medical professionals. It aims to offer comprehensive intervention solutions for cerebrovascular diseases, including ischemic stroke, hemorrhagic stroke, and intracranial vascular stenosis.
Cookies
Please note that your use of this website is governed by your acceptance of our Terms of Use. We also use cookies on our website to understand the usage patterns of visitors, so that we may be able to enhance their browsing experience and improve the website and/or our services. We may also allow certain third parties to place cookies on our website to collect information about your online activities on our website and across different websites you visit over time. Please click here for more information about our Cookie Policy.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.